
Dr. Anam Tariq continues the CKD discussion. In this part she discusses the diabetic kidney disease (DKD) and the following topics:
In this video we will learn about :
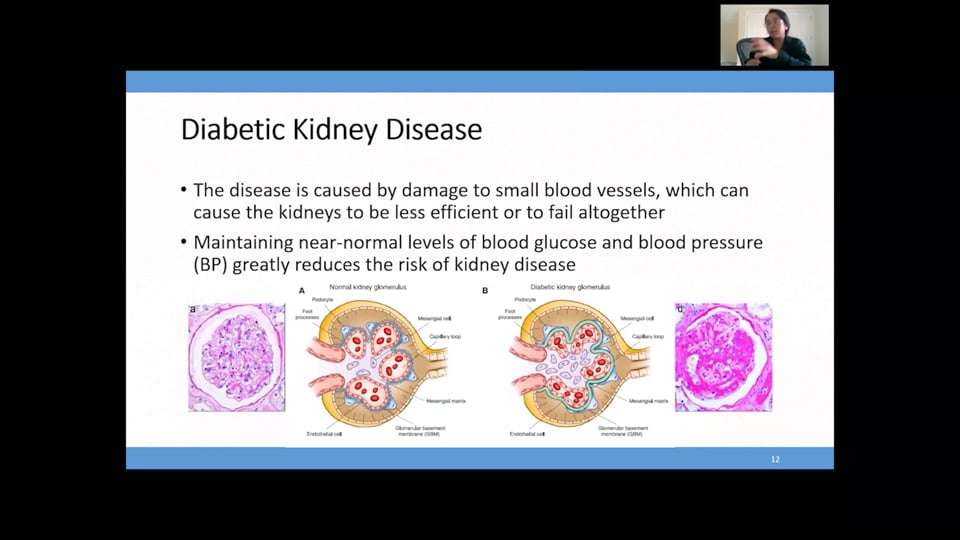
1. Diabetic kidney disease (DKD).
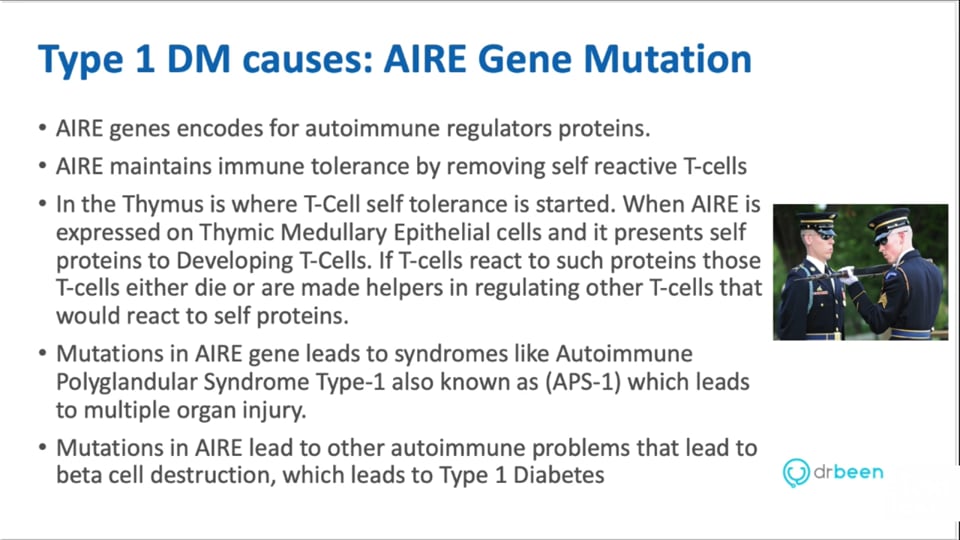
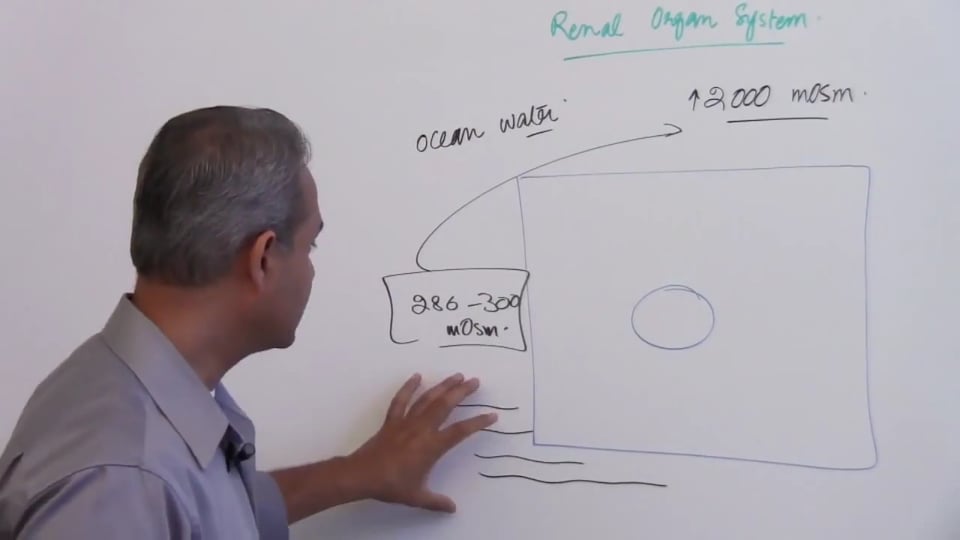
2. Pathophysiology.
3. Modifiable and non modifiable risk factors
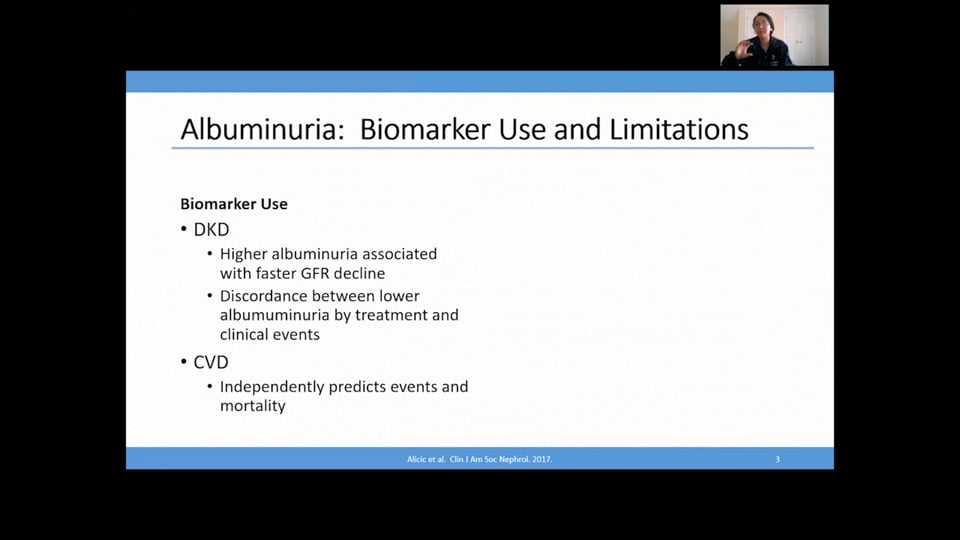
4. Diagnosis of DKD.
5. Sages of DKD.
6. Treatment.
7. Factors that affect CKD progression.
8. Blood pressure control in CKD.
9. Dose adjustment in CKD.
Following answers are created by ChatGPT. Occasionally the answer may be harmful, incorrect, false, misleading, incomplete, or limited in knowledge of world. Please contact your doctor for all healthcare decisions. Also, double check the answer provided by the AI below.
No credit card information needed.
 1.75 CME
1.75 CME
Amr Madkour, MD
Ahmed Zaafran, MD
 1.25 CME
1.25 CME
Dr. Mobeen Syed
 1.25 CME
1.25 CME
Dr. Mobeen Syed
Dr. Anam Tariq
Dr. Anam Tariq

Dr. Anam Tariq
John Prietto
Dr. Mobeen Syed
Dr. Mobeen Syed
 0.17 CME
0.17 CME
Dr. Mobeen Syed
 0.17 CME
0.17 CME
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed

Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
Dr. Mobeen Syed
All information contained in and produced by DrBeen corp is provided for educational purposes only. This information should not be used for the diagnosis or treatment of any health problem or disease.
THIS INFORMATION IS NOT INTENDED TO REPLACE CLINICAL JUDGMENT OR GUIDE INDIVIDUAL PATIENT CARE IN ANY MANNER.
Click here for notice and disclaimer.
Write A New Comment
2 Comments
srtupper@*.com
Nov 23 2020, 7:51 pm
If I have a pt who requires treatment for HTN and they look like they may progress to DKD at some point (i.e. uncontrolled diabetes), would it be a good choice to just start them right out on Losartan? I know amlodipine is 1st line therapy in many patients. Thanks for your thoughts and for a great lecture.
Sarah
asharma@*.com
Sep 16 2020, 3:29 am
HOW DO YOU TREAT HYPERPHOSPHATAEMIA IN CKD?WHAT ABOUT HYPERPARATHYROIDISM?